
Other names: Radial hemimelia, Radial Club Hand, Radial Dysplasia
Radial longitudinal deficiency is a rare condition that affects the forearm, and can affect one or both arms. It is sometimes called radial club hand, radial dysplasia, or radius deficiency.
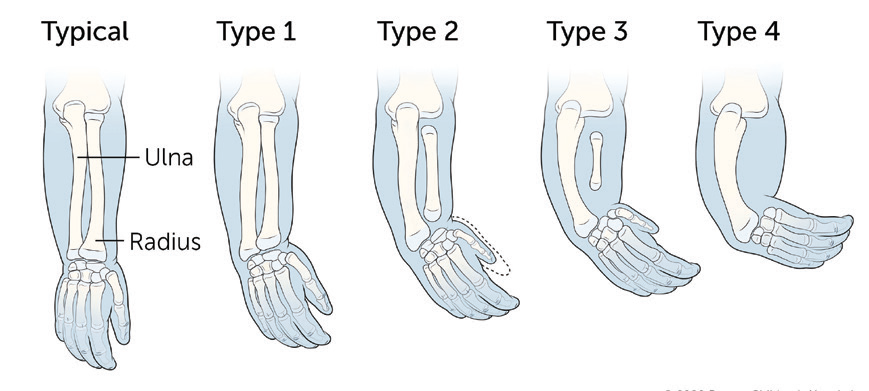
There are two bones in your baby’s forearm: the ulna, on the outer side of the arm, and the radius, on the inner side. Radial longitudinal deficiency occurs when the radius does not form properly. This causes the wrist to bend toward the thumb side of the forearm.
Radial longitudinal deficiency also affects the soft tissues and flesh of the forearm. The arrangement of muscles and nerves may be unbalanced, and some muscles and nerves may be missing. The thumb may be absent or smaller than usual with poor joints and missing muscles and/or tendons.
What causes radial longitudinal growth disturbance?

Radial longitudinal deficiency usually occurs by chance, although for some people it can also run in the family. Doctors and scientists do not know why some children are born with this condition.
There are no known links between this condition and the parent’s lifestyle or anything the mother may do during pregnancy. Radial longitudinal deficiency can be associated with several congenital syndromes, including those affecting the heart, digestive system, and kidneys.
How is Radial longitudinal growth disturbance treated?
All children will adapt to their own situation remarkably well as they grow and develop their manual skills. They will find solutions to most tasks expected of them. The aim of any surgery is to make those tasks easier to achieve.
There are various options for treatment and the specialist doctor will explain which are most suitable for your child. This decision about suitable treatments is influenced by the severity of your child’s radial club hand and their general health including other symptoms. It also depends on you and your family’s feelings about treatment, as some options involve a number of operations and quite involved care at home, which will require determination from all involved.

It is not possible surgically to restore a normal hand and forearm. However, it is possible to make the forearm straighter, and longer and to realign the wrist.
Non-surgical hand therapy and splints
Non-surgical treatment with stretches and splints is usually required in all types of radial club hand.
In mild cases, early in infancy, you will be shown a series of stretching exercises to carry out on your child’s wrist with the aim of increasing the range of movement.
In more severe types of radial club hand, stretches and splints are used. These are used before surgery to stretch the soft tissues. Splinting is also used after surgery to help maintain the corrected wrist position.
Surgery
A series of operations is sometimes recommended to those children with type ll, III and IV radial club hand, where a straightening of the wrist may be considered helpful for functional and cosmetic reasons. Surgery tends to take place in phases. There are also some operations that are best done when a child is at a certain age. Your doctor may suggest the following operations:
Distracting the soft tissues of the wrist with an external fixator

This aims to correct the position of the wrist and is normally planned for when your child is walking, usually at around two years of age. There are two parts to this procedure. The first part involves surgery to attach an external fixator (a metal bar or frame) to your child’s forearm and hand bones. After the operation, the soft tissues are gradually stretched – this process is called distraction. The two pieces of the external fixator are gradually moved apart to straighten the wrist, usually by a millimetre or so each day. Once the distraction phase has finished, the fixator needs to remain in place for several more weeks while the bone grows stronger and the tissues remain stretched. During this time, you will be expected to help clean where the pins come through the
skin and to perform the distraction. You will be supported and trained in how to do this and you will need to be seen regularly in the hospital to check that all is going as planned. The process of distraction is lengthy and demands commitment from you and your child. The usual time that the distractor is on
the arm is between eight and twelve weeks.
Re-positioning the hand
This is an operation to remove the fixator and maintain the new position of the hand sitting on the end of the ulna bone. This will either be achieved by a tendon transfer for a ‘radialisation’ operation where movement is preserved, or a tendon transfer and bone fixation for a ‘centralisation’ operation, where
most of the wrist movement is lost, but the wrist is fixed in a better position for function.
The bending of the wrist can recur as the child grows older and may require further surgery. For this reason, all children require follow up until adulthood when growth has finished, and the growth of the arm and hand are stable.
Forearm lengthening
Most children with radial club hand have short forearms in the limbs affected. There are operations that can be used to lengthen the forearm but these are complex and rarely produce forearms of the same length. If surgery is possible, this would be offered during mid to late adolescence.